
Herein lies the core learning dilemma…
we learn best from experience but we never directly experience the consequences of many of our most important decisions.— Peter M. Senge, The Fifth Discipline.
The transfer of learning is defined as the use of past learning when encountering new information and the application of that knowledge to both similar and novel situations.
Transfer, after all, is the whole point of education.
Yet, the literature in the learning sciences show, transfer is extremely hard to achieve.
Maybe we are skilled at “transferring” knowledge for tests and exams. But we are dismal at transferring it to the real-world.
For example, one would hope that informal reasoning skills would improve after studying in a university. In a study looking at this, fourth-year college students were no better than first-year college students. Fourth-year grad students were barely better than first-year grad students. In other words, students barely improve at reasoning ability about everyday events. People with better reasoning ability at the outset, not because of the higher education that they received.[1]
Author of Transfer of Learning, Robert Haskell states,
In effect, what the majority of studies show isn’t a failure of students to achieve transfer of learning but something worse: a failure of learning itself…Without exaggeration, it’s an educational scandal.
Transfer of learning is paradoxical. It’s there all the time in our everyday lives, but when we want it, we don’t get it.
This includes our continuous professional development (CPD)/ continuing education (CE) efforts.
Greg Neimeyer and colleagues point out that for the most part,
there is a lack of empirical evidence that CE is effective in improving clinical practice.[2]
Is this really true? I mean, wouldn’t we know so if our efforts are not translating?
Let’s look at five relatively recent studies that seek to examine the effects of training.
1. Skills After Two Years of Training
Tim Anderson and colleagues looked at a sample of 23 therapists in a university psychology clinical who saw 65 graduate students.[3] These therapists had two years worth of doctoral-level clinical psychology training. They prospectively saw their clients for seven weekly sessions.
An “untrained” group of 12 doctoral students from various non-clinical disciplines (Biology, Chemistry, History, and Communications), who had no prior clinical training, also engaged with clients for the same duration.
What did they find?
The untrained group achieved client outcomes comparable to those of the doctoral students in clinical psychology.
What the researchers found was that facilitative interpersonal skills (FIS), a skill rating of one’s therapeutic relational ability, predicted alliance and outcomes.
In other words, some therapists have higher FIS scores, whether they are from the trained or untrained group.
Further evidence support the validity of the FIS ratings. High FIS therapists also had higher client-rated alliances from the first sessions and significant improvements on alliance than low FIS therapists.
Another prospective study from Tim Anderson and colleagues found similar results.[4] Trainees’ interpersonal skills, as measured by the FIS before commencing their graduate training, predicted their ability to help clients.
Taken together, it does beg the question: Did transfer of learning from training into the real clinical world, happen for these trainees?
Based on these two studies, the answer seems to be no evidence of it. One might even suspect that the ones who got good at what they do, got it from elsewhere outside of their formal training.
RELATED
- See our DCT Study, which also employed the use of the FIS: Improving Responses to Challenging Scenarios in Therapy.
- What I’ve learned from the DCT project.
2. Therapist Effects on Outcome: Meaningful Differences Exist Early in Training
Here’s another study.
While differences between therapists are well-established (i.e., 5-9% of the variance is due to therapist effects), their presence of it at the earliest stages of a therapist career is less known.
Chris Edmondstone and colleagues conducted a study with 35 therapists that saw 202 clients at an outpatient training clinic, examining if therapist effects are present even from the beginning.[5]
What did they find?
Even after controlling for effects related to differences in theoretical orientation,
therapists-in-training differed in significant ways as measured by the average magnitude and rate of change of clients in their caseloads, as well as clients’ end-of-therapy clinical classification.
In short, differences between therapists exist even before training took place.
This echoes what Tim Anderson et al. found as well.
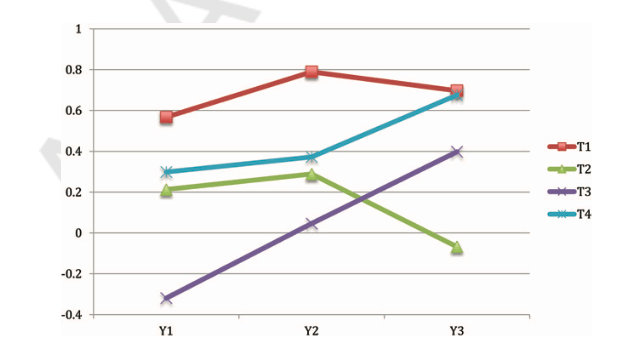
Comparing the differences in client outcomes, the top-10 therapists had 46.2% recovery rates, compared to 15.9% for the bottom-10 therapists.
See the graph below for further comparisons in improvement, no-change, and deterioration rates.

Given that meaningful differences between therapists exist as early as 2-4 years of training—especially between the best and the worst performing therapists—the authors of this study raise an important consideration. They conclude that the use of routine outcome monitoring represents an “ethical imperative.”
They add,
…to ignore the information provided by these tools would be a disservice to trainees.
Question: In your part of the world, do clinical supervisors know how the caseload of their supervisees are doing?
3. Does Training Improve Client Outcome
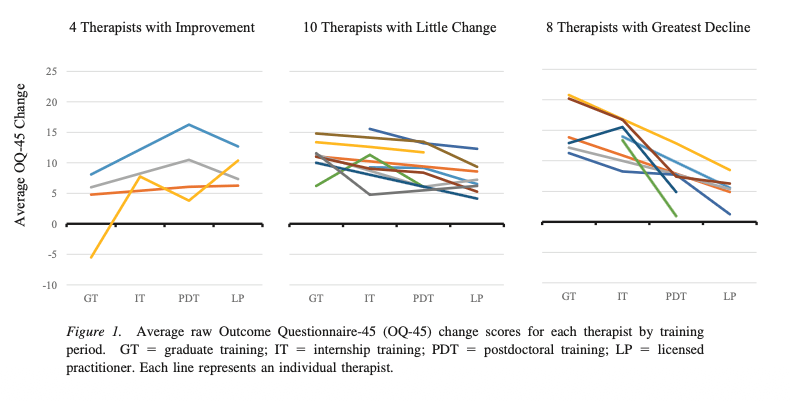
In this next study, David Erekson and colleagues conducted a longitudinal investigation on the impact of psychotherapist training.[6] Their study consists of 22 PhD-level psychologists who have seen a total of 4,047 clients.
In essence, there were asking a direct question, “Does training improve client outcome?
Here’s what Erekson et al. found:
- Therapists were found to achieve the same amount of change on average in their later stages of training.
- Findings suggest that as therapists progress through formal stages of training, they do not improve in their ability to effect change in their client.
- Granted, some do improve with training. But in essence, psychotherapy training does not have a universal effect.
Upon visual inspection of the data, only 4 out of 22 (18%) of the therapists improved over time. Most (82%) had little difference or even got worse over time.
l. [7]This finding is consistent even with more experienced therapists by Simon Goldberg et al. [7], followed by a German replication study. [8] Both studies found that experience did not lead to improvement over time.
RELATED

4. As Good As It Gets?
Finally, in a similar vein, Jesse Owen and colleagues studied if trainees in the US improved in their clients’ therapy outcomes over time, or, if it is “As good as it gets?”[9]
Here’s what Owen et al. found:
- Trainees improved over time, but only with clients who are less distressed.
- There was no change over time when working with more distressed clients.
- Some improved over time, while others declined.
- There was no universal effect from psychotherapy training.
The Pressing Issue
Taken together, what do we make of these findings?
It’s clearly not because of a lack of trying.
I have not met a therapist who said to me, I’ve made it. I’m enlightened. No need for development anymore.
It might not seem like the most pressing issue, but I believe that, for starters, if we re-imagine how we conduct clinical supervision, we stand a fighting chance to turn things around.
At the heart of our work, it is people passing on to other people. Clinical supervisors passing on to therapists, therapists passing on to clients.
This is the way we transfer our gifts to others.
Tapping Into Native Wisdom
Given what we know so far from the handful of studies we’ve highlighted about the impact of training—or the lack of—as well as the apparent differences to between therapists from the get-go, instead of hyper-fixating on the “common-core” competency skills we need to acquire, we need to consider what it means to tap into what each individual healer has to offer, and bring that to the table from the very beginning.
Let’s call this native wisdom.
Native wisdom is located in our prior knowledge, our existing story, experiences and relational encounters that consist of both pains and sparks in our history.
Educational psychologist David Ausubel said,
If I had to reduce all of educational psychology to just one principle, I would say this. The most important single factor influencing learning is what the learner already knows. Ascertain this and teach him accordingly. (emphasis mine).
This is relevant to clinical supervisors. Our role is to tap into the existing knowledge of each supervisee, and then, help them cultivate what they already have.
Nature is designed to be nurtured.
RELATED:
Transfer Redux
Perhaps one of the most important things we can do is to adopt what Robert Haskell calls the “spirit of transfer.”
For us in the field of therapy, this means that we need to close the loop by systematically monitoring if our training efforts actually leads to better outcomes for those we seek to serve.
Without this spirit of transfer, we are likely to achieve the same results as what these studies found: a lack of improvement over time.
But there is hope.
Nick Cave said hope is optimism with a broken heart.
We must learn to let go of our old ways that doesn’t improve our client’s lives.
Footnotes:
[1] Perkins, D. N. (1985). Postprimary education has little impact on informal reasoning. Journal of Educational Psychology, 77(5), 562–571. https://doi.org/10.1037/0022-0663.77.5.562 (article link)
[2] Taylor, J. M., & Neimeyer, G. J. (2017). The Ongoing Evolution of Continuing Education: Past, Present, and Future. In T. Rousmaniere, R. Goodyear, S. D. Miller, & B. E. Wampold (Eds.), The Cycle of Excellence (1st ed., pp. 219–248). Wiley. https://doi.org/10.1002/9781119165590.ch11
[3] Anderson, T., Crowley, M. E. J., Himawan, L., Holmberg, J. K., & Uhlin, B. D. (2015). Therapist facilitative interpersonal skills and training status: A randomized clinical trial on alliance and outcome. Psychotherapy Research, 1–19. https://doi.org/10.1080/10503307.2015.1049671
[4] Anderson, T., McClintock, A. S., Himawan, L., Song, X., & Patterson, C. L. (2016). A prospective study of therapist facilitative interpersonal skills as a predictor of treatment outcome. Journal of Consulting and Clinical Psychology, 84(1), 57–66. https://doi.org/10.1037/ccp0000060
[5] Edmondstone, C., Pascual-Leone, A., Soucie, K., & Kramer, U. (2022). Therapist effects on outcome: Meaningful differences exist early in training. Training and Education in Professional Psychology. https://doi.org/10.1037/tep0000402
[6] Erekson, D. M., Janis, R., Bailey, R. J., Cattani, K., & Pedersen, T. R. (2017). A longitudinal investigation of the impact of psychotherapist training: Does training improve client outcomes? Journal of Counseling Psychology, 64(5), 514–524.
[7] Goldberg, S. B., Rousmaniere, T., Miller, S. D., Whipple, J., Nielsen, S. L., Hoyt, W. T., & Wampold, B. E. (2016). Do psychotherapists improve with time and experience? A longitudinal analysis of outcomes in a clinical setting. Journal of Counseling Psychology, 63(1), 1–11. https://doi.org/10.1037/cou0000131
[8] Germer, S., Weyrich, V., Bräscher, A.-K., Mütze, K., & Witthöft, M. (2022). Does practice really make perfect? A longitudinal analysis of the relationship between therapist experience and therapy outcome: A replication of Goldberg, Rousmaniere, et al. (2016). Journal of Counseling Psychology. https://doi.org/10.1037/cou0000608
[9] Owen, J., Wampold, B. E., Kopta, M., Rousmaniere, T., & Miller, S. D. (2016). As good as it gets? Therapy outcomes of trainees over time. Journal of Counseling Psychology, 63(1), 12–19. https://doi.org/10.1037/cou0000112


1 Response
[…] What are the most pressing problems in the practice of psychotherapy? […]