Note: This is a compilation of Frontier Friday, a weekly Substack published, originally released on 26 Aug. 2022
PART I
As a child, my uncle used to perform magic tricks for my cousins and I. What a thrill to see things disappear out of thin air and reappear behind our ears. He was a really good entertainer (He’s a master puppeteer now). Later in life, I learned a bit about magic. I had a friend in school who became a close-up magician (I wrote about this here). But the thing is, as the great magician Jamy Ian Swiss noted, it’s easy to figure out how a trick is done, but the real difficult part is to develop the art of doing it.
What has this got to do with psychotherapy?
Knowing about how the therapeutic alliance works is quite different from how it’s done in the conversational reality and healing space of therapy.
In the late 1930s, a young psychologist noted the following:
This was none other than Carl Rogers.1
As you plunge in to this topic of Working Alliance in the coming weeks of Frontiers Friday, I urge you to do the following:
- Write down what you currently know about therapeutic alliance (alliance predicts outcomes, etc.). Elaborate as much as you can,
- Read each of the recommendations made, or at least the summaries I provide in this series, and finally,
- Note down how does the new input connect with your prior knowledge2.
- 📽 New Video from Frontiers, Therapy Tip of The Week: Embodied Cognition
It’s easy to get lost in our heads. Our pet theories end up dominating and preventing us from being in touch with the person in front of us.
In Part 3 Therapy Tip of the Week, I’d talk about how psychotherapists can employ the principles of embodied cognition—the idea of embodiment as a way of thinking—to help you deepen your empathic understanding of your clients, especially in stuck situations. - ✍️From the Frontiers Archives: What Therapy Is (Or Isn’t).
The psychodynamic camp says, “Your past is the problem.”
The third wave mindfulness therapist says “Mindlessness is the problem.”
The emotion-focused therapist says, “Your unresolved feelings are the problem.”
The pioneering team at Mental Research Institute (MRI), Palo Alto says “the attempted solution is the problem.”
The solution-oriented practitioner says “There are exceptions to the problem.”Pre-deciding what the problem is, is the problem. And just maybe, focusing on the engagement with each person is the way. - 👀 Visual: How Much Does Alliance Contribute to Treatment Outcomes?
To put into perspective, how much does alliance contribute to outcomes, relative to other factors?
The answer: Based on a wealth of studies published over the last four decades, therapeutic relationship exerts about 5-8%, whereas models and techniques contributes about 1%.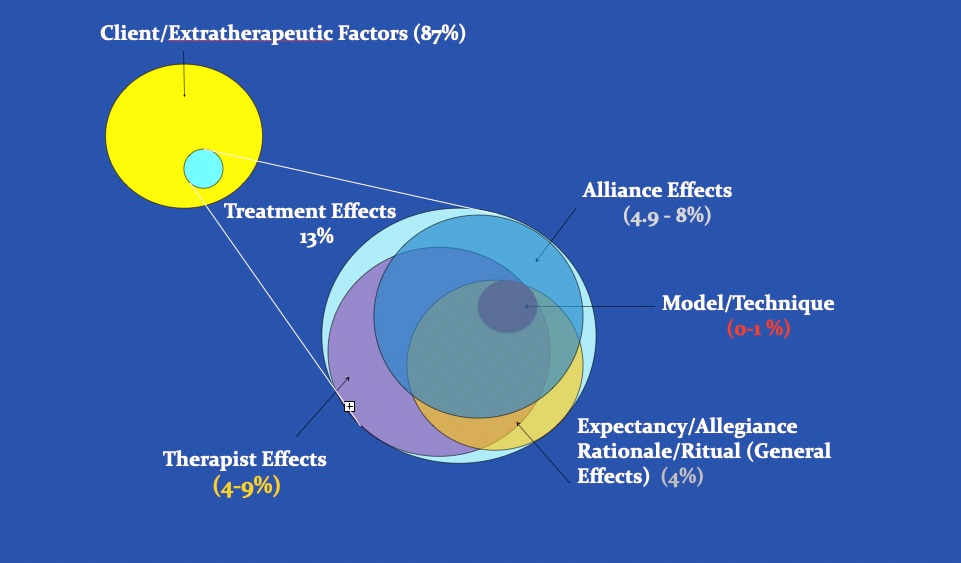
- 📜 Research: It’s Not Just High Alliance
In one of the largest study (2990 youths treated by 98 therapists) on the role of alliance in the treatment of adolescents–even larger than the number of all the samples combined in a meta-analysis (McLeod, 2011)–my colleagues and I found that alliance ratings that improve over time is more predictive of outcomes than alliance at a given point in time (i.e., mono-assessment model), or an aggregation of multiple alliance points (i.e., aggregate-assessment model), which most alliance-outcome studies tend to utilise.As counter-intuitive as it seems, lower initial alliance ratings that improves over time (i.e., low to high) is more predictive of good outcomes than high alliance ratings over time (i.e., high to high). Large changes in scores (from low to high) on the SRS across sessions accounted for 10% of the variance in outcomes compared with 1% for alliance scores that started either high or low but remained stableImplication: Learning to elicit nuanced feedback early on is key.(Also Available on ResearchGate) - ⏸ Words Worth Contemplating:
”We’ve lost the ‘care’ in healthcare.”
~ Ai-jen Poo, author of The Age of Dignity.
Reflection:
How do we preserve the dignity of care in our work?
As a point of reflection, what do I need to do with my relationship with time, so that I am less hurried in my conversations?
As the late writer and poet John O’Donohue pointed out, stress is our perverted relationship with time.
PART II
- 🎥 New Video from Frontiers, Therapy Tip of The Week #4: The Devil is in the Details Between Sessions
In this week’s Therapy Tip of the Week (TTW), I address a subject that you as a psychotherapist would be more than familiar with—except that it’s not what you expect.
- 👓 Read: The Definition of Working Alliance
What constitutes as working alliance has lasted almost as old as I am. Alliance is more than just about emotional connection. According to Edward Bordin’s 1979 article, working alliance has been defined as
i. Relational bond
ii. Agreement on the goals, and
iii. Agreement on the means, methods and tasks to reach those therapeutic goals.
There are significant implications to operationalising this in therapy. For instance, an agreement of the goals and direction of therapy has a huge impact on treatment outcomes, or the lack of.
(See Related post: What Are the Perennial Pillars for Psychotherapists?)
And you could be doing what is the cutting edge of “evidence-based practice,” but if it doesn’t sit well with your client, you are more likely to have a poor working relationship, and thereby increase the odds of dropout.
(Dropout is a topic we will cover in-depth in future series of Frontiers Friday, so be so to subscribed if you haven’t already.) - 📜 Research: Facilitative Interpersonal Skills as a Predictor of Therapist Success
This landmark study in 2009 opened up the doorway to our understanding of therapists’ ability contributing to alliance formation. Tim Anderson and colleagues found that therapists’ facilitative interpersonal skills (FIS), the ability to perceive, understand and communicate impactfully, accounted for variance of outcomes between therapists.
Said in another way, FIS accounted for variance in outcomes due to differences in therapists abilit to handle challenging situations. Tim Anderson et al’s FIS study was a real inspiration to our Difficult Conversations in Therapy (DCT) project. (More on DCT in the coming future.)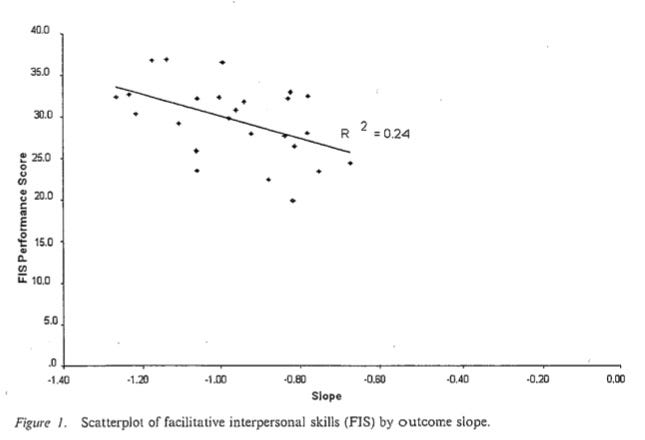
- 📜 Research: Therapist facilitative interpersonal skills and training status: A randomized clinical trial on alliance and outcome
As a follow-up study, Tim Anderson and colleagues published a fascinating paper in 2015 (the authors made this available in Researchgate).
They found that a therapist’s relational ability before attending graduate school, was a significant predictor of outcomes and alliance formation. The impact of training was “negligible”. In other words, a 2-year relevant doctoral training had no significant effect on client outcomes. Intriguingly, though not statistically significant, untrained therapists had higher alliance ratings! In other words, there is a possibility that a trainee’s ability prior to receiving any training, matters more than the effects of training. So, the real question we should be asking is, what the heck are we doing in our training programs? - ⏸ Words Worth Contemplating:
“When our hearts are small . . . We can’t accept or tolerate others and their shortcomings, and we demand that they change. But when our hearts expand . . . We accept others as they are, and then they have a chance to transform.”
~Thich Nhat Hanh
Reflection:
How is my heart? (Take a moment of pause)
What do I need to do to teach my heart to be open and expansive?
What areas do I need to soften, and not harden?
PART III
- 🎥 New Video from Frontiers, Therapy Tip of The Week: Seek to be Disconfirmed
Dissonance can be a powerful ingredient for learning. How do we challenge our intuition in order to listen to our client’s unspokens in order to foster a deeper connection with them?
In this video, I recommend an exercise that I use called the “Rate and Predict,” to help me open up the conversation in therapy.
- 👓 From the Frontiers Archives: To Understand? Easy. To Help Someone Feel Understood? Difficult.
The tough part is to help someone feel understood. This is why I strongly believe we need more direct training in the conversational nature of therapy, much more than the emphasis that we place in theoretical understanding especially at the early stages of our career. - 📜 Research: The Alliance-Outcome Association in Couples Therapy
I mentioned this in issue FF41. This study was conducted in Singapore. We found that from a shared influence model was a significant predictor of therapy outcomes. Even though each partner were rating their alliance experience with the therapist, there was a shared experience.
I know, this isn’t earth shattering news. This is something systemic thinkers have previously conceived the couple-hood as an entity, and understood that both parties have an influence on the other. This is also makes couples therapy more challenging (and rewarding).
- 📜 Research: Socioeconomic Status and the Therapeutic Alliance
I suspect that we don’t fully appreciate how much SES affects a wide variety of life factors, such as physical health, mental health, cognitive ability.
When I read this paper, I was still somewhat taken aback that SES also affects the engagement levels in the therapy room.
These researchers from Sweden found that clients of lower SES, on average, felt less understood and inferior to their therapist, “as well as possible perceptions that such client(s) are less suitable for psychotherapy.”
This was more pronounced in a psychodynamic context than CBT treatment approach. This study has prompted me to include SES (and maybe even perceived SES if I might add that in my pre-therapy questions) as a factor to consider in my future outcomes analysis. - ⏸ Words Worth Contemplating:
“It takes two to know one.”~ Gregory Bateson
Reflection:
Two-Parts
Part I:
Who makes you feel understood?
Picture this person in front of you. What does that feel like? How does this person relate with you that makes you feel warmth?
Part II:
Are they people whom you see who are economically disadvantaged or are on the margins of society? Picture them in front of you.
How do you think they experience you? How do you equalise the ground so that they might feel less inferior to you?
PART IV
- 🎥 New Video from Frontiers, Therapy Tip of The Week #6: How to Elicit Nuanced Feedback

In Therapy Tip of the Week #6, we continue on the topic of improving working alliance. Here’s my recommendation: When seeking for feedback, avoid talking about… you! If you have missed the previous videos on how to improve working alliance, here are links:
i. Seek to be Disconfirmed
ii. The Devil is the Details Between Sessions
⏳ Time Stamps:
00:00: Introduction
01:00: Using Depersonalised language
01:42: What Feedback is Not
02:02: Feedback to Feed-Forward
04:14: Summary - 📜From the Frontiers Archives: To Be Altered
Turns out that our willingness to be changed affects clients’ outcome. - 📜From the Frontiers Archives: What Does General Athleticism Got to Do With Psychotherapeutic Skills?
What are the implications if alliance ability is like your general fitness in any sports? - 👓 Research: Untangling the Alliance–Outcome Correlation: Exploring the Relative Importance of Therapist and Patient Variability in the Alliance
Not the most appealing title, but dismantling studies are super useful for us to understand what’s really going on under the hod.
This 2007 study is a landmark study. Baldwin, Wampold and Imel were able to untangle the alliance-outcome correlation, and what they found was that a staggering 97% of the differences in therapist outcomes was explained by therapist’s alliance ability!
(This type of numbers are usually unheard of in social sciences).
In other words, some therapists have this relational ability to engage with a wide variety of people.Note: This figure from the study illustrates that differences in alliance, leading to improvement in symptom reduction, is due not to the differences within a therapist’s caseload, but due to the differences between therapists. In other words, some therapists were much better at alliance formation.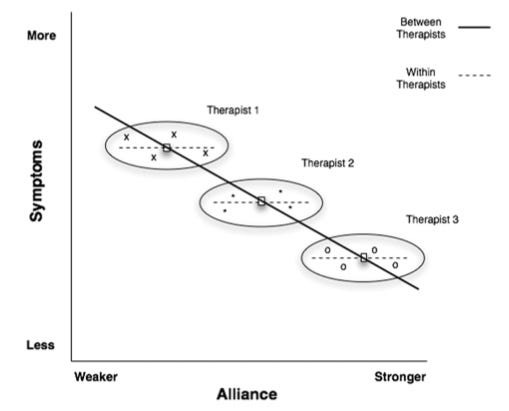
- ⏸ Words Worth Contemplating:
“Our intention is to affirm this life, not to bring order out of chaos, nor to suggest improvements in creation… But simply to wake up to the very life we’re living.”
~ John Cage.
Reflection:
When was the last time you’ve changed your mind?
What was it about?
Train your mind to be willing to be altered, to be updated, to learn.
Write them down, number and date them.
Make it a habit to look back at them.
A measure of success is how embarrassed you feel of yourself a year ago.
PART V
- 📽 New Video from Frontiers, Therapy Tip of The Week #7: How to Use Measures Less Like an Assessment Tool, and More Like a Conversational Tool
- In this week’s Therapy Tip of the Week #7 (TTW), I talk about how to use outcome monitoring tools, not as an assessment tool, but as a conversational tool.
Sidenote: There are backfire effects if we use measures purely as an assessment tool. See this: The Tyranny of Metrics - ⭕️ From the Frontiers Archives: How to Receive Feedback & How to Get Better at Eliciting Feedback
We talked about this in issue FF35, when we were discussing about Feedback-Informed Treatment (FIT).
This has direct implications on how we can directly calibrate in real-time so as to develop better alliance. - ⭕️ From the Frontiers Archives: To Get Useful Feedback, Seek Contrast
Don’t underestimate the power of being cognisant of the previous session’s engagement level.
In this blogpost, I talked about how you can use feedback and feed-it-forward, so that you can learn responsively adapt to each client. - 👀 Research: Therapist Alliance Activity, Therapist Comfort, and Systemic Alliance on Individual Psychotherapy Outcome
Jesse Owen has been a great collaborator. In this 2015 article with Norah Slone, they examined the systemic influence of alliance in individual therapy on outcome.
Key Grafs:
Client outcome improves when- Therapists overtly checked in about the therapeutic alliance
- Therapists were rated as being more comfortable, and
- Clients’ social networks were aligned with goals and tasks of treatment.
- ⏸ Words Worth Contemplating:
“Remember: When people tell you something’s wrong for them, they almost always right. When people tell you exactly what they think is wrong and how to fix it, they are almost always wrong.”
~ Author, Neil Gaiman.
Reflection:
Not all feedback is created equal.
Who specifically do you trust to give you feedback about your development?
It’s important to distinguish between performance feedback and learning feedback.
Feedback from clients are performance feedback, used to specifically tune and calibrate to individual’s needs, one client at a time.
Feedback from a mentor/coach/supervisor are learning feedback, used to specifically help you with at your growth edge, one therapist at a time.
Yes, listen to to a crowd’s response if you are performing on stage. Their real-time responses give you a sense if you message, music or joke has landed. They can tell you what worked or didn’t, but they can’t tell you how to improve. Everyone will have a different opinion. They might even be able to tell you what’s wrong, but not how to fix what’s wrong.
Once again, not all feedback is created equal, even in terms of learning feedback. Be warned: What is guised as “feedback” is actually a performance “evaluation”.
Besides, an over-emphasis on performance can impede real learning.
In order for learning feedback to be useful, it has to be specific, targeted and contextually relevant. Theoretical discussions and affirmations aren’t learning feedback. While needed at times, they aren’t sufficient to lead to actual translation of better client outcomes.
(First appeared in Frontiers of Psychotherapist Development: The Guise of Feedback).
PART VI
- 📽 New Video from Frontiers, Therapy Tip of The Week #8, Listening for Changes in Wellbeing

Don’t be seduced by an approach of starting every session with “What’s gotten better since the last session?”
First, find out if things have gotten better. If things are still stuck in a rut, it would come across as unsympathetic and ignorant to be sticking to the formula of being “strength-based.”In this week’s tip, I’d talk about how we can specifically listen for changes between sessions, and why measuring a person’s wellbeing matters more than a symptom-specific measure. - 📜Research: The reciprocal relationship between alliance and early treatment symptoms: A two-stage individual participant data meta-analysis
A recent meta-analysis trying to sort out if alliance leads to improvement or improvement leads to better alliance.
Key Grafs:- Early alliance predicted post-treatment outcome.
- “…in the early phase of therapy, symptoms and alliance were reciprocally related to one other, often resulting in a positive upward spiral of higher alliance/lower symptoms that predicted higher alliances/lower symptoms in the subsequent sessions early in therapy.”
- 📜Research: Assessing the Alliance–Outcome Association Adjusted for Patient Characteristics and Treatment Processes”: A Meta-Analytic Summary of Direct Comparisons
Another meta-analysis.
This time the question is related to how much of client’s characteristics at intake, as well as therapist’ adherence and competence affects the alliance.
Key Grafs:- This study found that alliance-outcome association is an “independent process-based factor,” i.e., above and beyond client factors at intake.Based on the Supplementary Materials, it appears that there is a wide-range of variables consisting of “Intake factors” e..g., gender, age, symptoms and wellbeing measures at baseline.This was also the first meta-analysis to examine the effects of adherence and competence on the alliance-outcome association, which was found not to be a predictive factor.
- 📜Research: Within-patient perceptions of alliance and attunement
Sometimes I read research papers and I think I already know what they found. Don’t be misled by the simplicity of this recent 2021 study on therapeutic relationship.
Researches from US, Canada and Israel teamed up to figure out if differences in alliance between clients or differences within client (i.e., changes in alliance over time) predicted outcome. (Make a guess what the results are before reading on.)
Key Grafs:
i. “The general experience of a strong therapeutic relationship (i.e., collaborative working relationship and feeling attuned and responded to) relative to other patients did not appear to contribute to symptomatic change.” In other words, the patient’s average working alliance score did not predict outcome.
ii. Instead, “the patients’ specific fluctuations in working alliance relative to their own general experiences appeared important for subsequent symptomatic change 1 month later.” In other words, improvement in alliance scores over time predicted improvement in psychological functioning.
iii. Special note: The importance of real-time monitoring of therapeutic alliance.
The authors cited that,
“This may be particularly helpful for patients who have difficulty expressing disappointment or unhappiness with therapy or those who are overly compliant. Indeed, Samstag et al. (1998) have pointed out that patients may be reluctant to voice dissatisfaction directly to the therapist in sessions, even though the exploration of such negative feelings might be very therapeutic.”
- ⏸ Words Worth Contemplating:
“Authenticity is the daily practice of letting go of who we think we’re supposed to be…”
~ Brene Brown, The Gifts of Imperfection.
Reflection:
Forging an alliance with each and every one of our clients, as diverse as they are, day in day out, is hard stuff.
And try as we may, they are some people that we fail to connect with.
We must not push, chastise or judge our clients if they don’t fit into the doctrines of our knowledge.
You are a healer, but not everyone wants your healing.
We must not push, chastise or judge ourselves to be more than we are. But we must stand at the door and invite people to the house of healing if they choose to.
For some, the conversation must begin at the doorsteps.
Meanwhile, we must continue to learn deeply, slowly and patiently. We must tend to our personal learnings less like a builder and more like a gardener. A builder builds, until it is completed.
A gardener is never done. A gardener plants some seeds under some good soil, waters it consistently, prunes and adds more… The garden is shaped into being, and continues to evolve, depending on your care of it.
Tend to the garden of your learnings.
(If you are interested in this type of gardening/learning, check out Deep Learner)


Recent Comments