In a previous post, I’ve talked about the importance of Developing First Principles Before Methods.
I’ve also talked about the ways you can develop first principles from challenging situations, therapeutic mistakes, and guidance from a mentor (see the previous post),
But what is the process required for learning from and developing first principles? Why is this important?
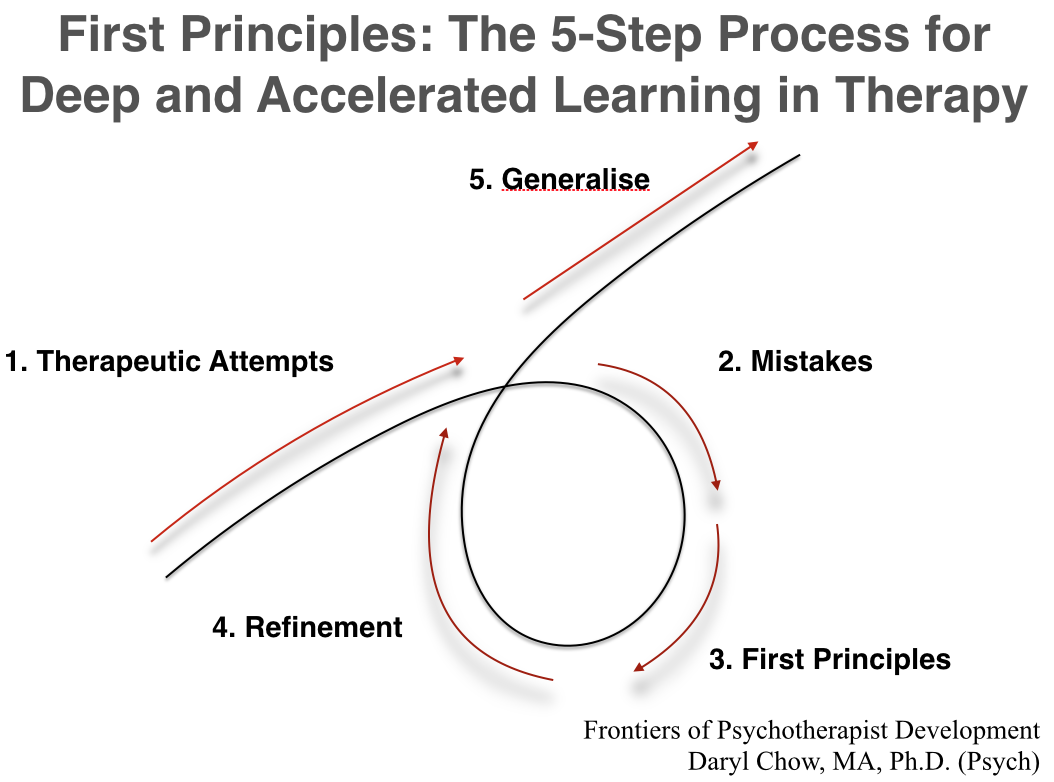
In this post, I’d spell out a 5-step approach (see Figure 1) to improve the rate of learning from your work, so that you can reap the rewards from your experience + reflection, and generalise the first principles to other related contexts:

Figure 1: The 5-Step Process for Deep and Accelerated Learning [1]
Step 1. Therapeutic Attempts:
At this stage, your focus is to perform to the best of your ability. Do what you do. It’s important to remind ourselves that if we can fully embrace what we have at a given point in time, it is enough. (Until you get to Step 5).
Step 2. Challenging Situations/Mistakes:
Catalog the various types of challenging situations that you’ve faced and the types of mistakes that you’ve made in the therapy hour. Name them, and make it a conscious attempt to revisit them. (See the previous post on points #1 & #2, Challenging Situations and Mistakes, respectively). Don’t leave this to chance. Block out some time in your calendar to do this.
It is important to remember, “It’s better to fail well than to succeed badly.”[2] This is not the most pleasurable activity to be doing, but just know that when you get through the five steps, it is very rewarding!
Step 3. First Principles:
Create space for deep reflection on the specifics. Distill the elements. Ask yourself, “what can you learn from this challenge/mistake?” Don’t get caught up in the technique or worry if you didn’t adhere well enough to a particular treatment protocol. Work backward (see Figure 2 of previous blog), and reflect on what was the underpinning idea that was guiding you in that situation. Turn that around, and ask yourself, “What might be a useful guiding first principle to adopt in this situation instead?”
Sometimes we come up with nothing at this stage. Read materials to spark off some ideas. Seek the help of a mentor/consultant/clinical supervisor to get some objectivity. We often miss the forest for the trees.
One time I was stuck with a case that just wasn’t going anywhere. In our group supervision, my supervisor noticed a certain pressure I was experiencing for driving the change in my client’s life who was steeped in depression. She offered me an idea that stuck with me for more than a decade on. Here’s what I’ve grafted from my supervisor’s suggestion and turned it into a first principle: “When a client is reluctant to commit to taking action, Raise the Possibility of Change vs No Change [3]

Figure 2: This is the post-it note that I’ve kept for many years to remind me of the lesson I’ve learned not to pressure for change, but to Raise the Possibility of Change vs No-Change.
Without establishing the roots of first principles, you are left to deal with challenging situations or mistakes in a haphazard fashion. Without first principles, you deal with each challenging situation or a genuine mistake as if you are experiencing it for the first time. Maybe that is one of the reasons we do not get better with experience.
Step 4. Refinement:
Guided by your first principles, this is the part when you repeat the scenario in your mind, or better yet, review the specific segment of the session recording, and try to improve on your attempts in that particular therapeutic engagement (see Step 1). Once again, this revised attempt must be guided by your newly developed first principle.
Here’s a clinical example to highlight the refinement process. Recently, I was working with a man in his 30’s who wanted to address his anger issues. Initially, I was guided by a first principle of figuring out the Client’s View of the Problem, given that it must be hard to acknowledge anger as a problem. But as we delved further about his “anger” issues, I soon realised that I wasn’t hitting the mark. I knew this because there wasn’t any resonance or vitality. The session was stale. It felt like each statement I made about his anger issues, my client was implicitly saying, “Yes, but…”
I thought about this before the next session. And it dawned on me I should go further and deepen on the issue he had with anger. I developed another first principle: Re-define the Problem. This idea meant that I should pursue what’s underlying the outburst anger towards his wife. So once we’ve established the focus at the start of the next session, I said the following to my client, based on the newly re-fined first principle: “You know, we talked about the issues with anger the last round. I want to hear what you think, but from what you’ve said, I don’t think that anger is the issue; feelingunappreciated is.”
Watching my client’s visceral reaction and listening to his response to that, he agreed with this. We came to a consensus that to be appreciated is an important theme to address in therapy. We found a way to acknowledge this issue with compassion, given that “un-appreciation”triggered a host of memories with his ex-wife. He was able to turn this around and found a way to have a conversation with his wife about to share about what happened in the past, and made a sincere apology to her for his recent outburst.
The reason for this clinical example is to stress the importance of the learning process, not the outcome of the session. I’m now able to extrapolate the newly minted first principle and use this concept in other situations. At first, I was guided by Client’s View of the Problem. In the process of Refinement, I revisited Step 3. First Principles, and re-framed it as Re-Define The Problem, which led to an emotional deepening and resonance for the client, and ultimately, meaning change in his relationship with his wife.
Step 5: Generalise:
This is the litmus test if your first principles are of any use. Use the first principle established in Step 3 & Step 4 and see if it helps you in other similar contexts. Be prepared to continuously refine and recalibrate. This tight feedback loop helps to accelerate your learning tremendously.

Imagine this feedback loop repeats itself in an iterative process, get better at each step of the way, cycle by cycle.
Talking about the concept of first principles is difficult. It is easily misunderstood as a rule, or even misconstrued as a new method. This is not my intention. It’s also not my intention to say that the first principles I’ve mentioned in the examples are the “correct” first principles to have.
Develop your own first principles. The purpose of developing your first principles is so that you can learn. Carl Rogers said, “The only person who is educated is the one who has learned to learn and change.”
At the heart of this 5-step Process for Deep and Accelerated Learning in Therapy, is to learn from our experience. Meaning experience is not what happened to you, but what you do with what has happened to you.
Remember the following:
LEARNING = THE ABILITY TO TRANSFER KNOWLEDGE INTO ANOTHER SITUATION.
I love to hear your thoughts around this 5-step process and the types first principles you’ve developed that guided you in your clinical practice. It might help to revisit the previous post on Developing First Principles Before Methods. Please leave your comments below and I will respond to you.
Best,
Daryl
Footnotes:
[1] My colleagues and I have been running the Difficult Conversations in Therapy (DCT) project that my colleagues over the last few years. Working with many therapists across several repetitions has allowed me to learn and develop this idea. We are now at a stage of near completion of an RCT, so more on this in the future posts. The idea for this diagram was adapted from one of the most important books I’ve seen this year, Principles, by Ray Dalio, founder of Investment company, Bridgewater.
[2] The original quote is from Cistercian monk, Thomas Merton: “A man who fails well is greater than one who succeeds badly.” No Man is an Island, p.127
[3] Some of you might think that this is a technique used in motivational interviewing. Maybe it is, but the idea is not to make it a technique, but rather to use it as a guiding first principle.


Daryl,
This is great! I eagerly await each of your blog posts! I am playing around with the question of how to develop a , “fist principles, deliberate practice” group supervision process at my agency. I’d like to develop the idea of creating a culture where this is the focus, rather than workshops on new techniques. Do you know of anybody doing this? Would make an interesting study, to implement something like this and track therapist development over time.
Thanks for all your work.
Cheers,
Joshua Taylor
hi Joshua, Thanks for your kind comments. You’ve hit on something important, that is creating a culture of effective focus in supervision. This is one of the reasons we developed the taxonomy of deliberate practice activities (TDPA) worksheet. (you have that yes? ) most of my consults and supervision start by helping individuals and teams figure out the WHAT before the HOW…. working on the key area that pays dividends towards outcomes.
Some studies are underway (e.g., in Norway). One paper was published in 2016 (Goldberg et al. 2016) documenting a similar (but very long) process. doi: http://dx.doi.org/10.1037/pst0000060 .
Would be interesting if you can turn your supervision group into a naturalistic study design!
Best,
Daryl
The most useful thing about this, I think is that it actually gives you a way of looking at the clients first principles… I think Milton Erickson was really good at this. He emphasized early learning experiences and translated those first principles to the clients current problem. I don’t think he teased it out like you have but he evoked the experience of learning, making mistakes, persisting and the magic was in the generalizing.
I am embarking on a project with a really tough community. These people don’t suffer fools gladly and have usually become disillusioned with mental health services, and I think rightly so. They know what doesn’t work for them and what makes things worse. A study comparing psychodynamic with CBT in such a population got generally bad results and blamed the clients for being “not sufficiently psychologically minded” GIVE ME A BREAK!
I thought I’d start by exploring their first principles. I have heard that when there is a crisis, like someone’s house burns down, they rally as a community. There will be some first principles there I think that can be generalized. I have worked a lot with individuals, say generalizing their Parental first principles to assist learning to ride a bike to assist their child learning to not hit when angry. It works because it is the clients first principles that are generalized I think. I think mental illness is a broken paradigm, and nowhere more so than these communities. People who get better in therapy would probably get better no matter who they see, but “therapy” is broken in these communities. It’s an unworkable paradigm I think.
We enjoyed your post so much! I like the fact that author explained the ideas.
I think it is merely as good as the article of these fellas
https://americansunrisepac.org. Thank you so much with
this article, I may wait for your following publications.