
PART I
-
 Research: A meta-analysis of outcome studies comparing bona fide psychotherapies: Empirically, “all must have prizes”
Research: A meta-analysis of outcome studies comparing bona fide psychotherapies: Empirically, “all must have prizes”
This is a seminal meta-analysis. This high-impact study had twice that of the next highest-cited relevant article in the Web of Science (WoS) citations.
Before this 1997 article, previous studies had not conducted true comparisons. Take, for instance, 8 out of 13 so-called “dynamic-humanistic” studies used for treatment comparisons did not actually contained therapeutic elements and “could be viewed as a straw man” (Shapiro & Shapiro, 1982, p. 591).Also, comparing with a wait-list or no-treatment, isn’t exactly good enough. Something is often better than nothing.
Wampold et al. define what a “bona fide” psychotherapy comparison:
“…those that were delivered by trained therapists and were based on psychological principles, were offered to the psychotherapy community as viable treatments (e.g., through professional books or manuals), or contained specified components.”
Key Graf:
– “The results of our analysis demonstrated that the distribution of effect sizes produced by comparing two bona fide psychotherapeutic treatments was consistent with the hypothesis that the true difference is zero.”The effect size for the comparison of bona fide psychotherapies is in the interval of .00 and .21.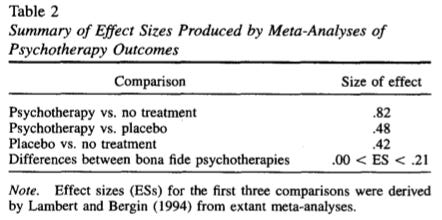
-
 Commentary: Brave new world: Mental health services 25 years since Dodo and 25 years in the future
Commentary: Brave new world: Mental health services 25 years since Dodo and 25 years in the future
Here’s Wampold commenting on their article in 1997.Key Graf:
– “I am skeptical of improving services by implementing purportedly superior treatments in a system of care, based on a randomized clinical trial, because
(a) the results often defy reasonable explanations,
(b) implementing results from clinical trials in other contexts is fraught with difficulty,
(c) psychotherapy trials rarely if ever are replicated,
(d) differences among therapists, due to their clinical skills, are more important than differences among treatments, even if a treatment is demonstrably (but marginally) better, and
(e) such implementation reduces therapist and patient preferences and leads to therapist discouragement.
– The designation of the RCT as the gold standard of psychotherapy research has set us back decades—to wit, identify one clinically actionable conclusion from RCTs, which by the way have cost hundreds of million of dollars.”
-
- Commentary: Smaller effects matter in the psychological therapies: 25 years on from Wampold et al. (1997)
Michael Barkham highlighted an interesting point about the value of systematically monitoring outcomes:– “Consider a recent large meta-analysis reporting an overall ES d of 0.15 for routine outcome monitoring, increasing marginally to 0.17 for patients not-on-track (de Jong et al., 2021).
– While classed as a small effect, it is additive to the existing overall effect of psychotherapy (i.e., it is an effect over and above the general effect of psychological therapies).”
-
- Commentary: The implications of the Dodo bird verdict for training in psychotherapy
Given my struggles in the formal education process, training and learning is one area I deeply care about.
Henny Westra raises some unsettling findings about the current state of training in the field of psychotherapy:– “there is no evidence that continuing education workshops… produce sustained skill development—quite the opposite.
– Large effects on self-report are found but any modest improvement in performance erodes over time without further coaching.”
-
 Words Worth Contemplating:
Words Worth Contemplating:
“It’s not enough to rage against the lie. You’ve got to replace it with the truth.”
~ Bono, U2.
Reflection:
Take another look at the Table above taken from The Great Psychotherapy Debate. What strikes you?
Where have you been investing your time, money and effort in your professional development?
PART II
-
- Watch: The Psychotherapy Debate with Peter Fonagy and Bruce Wampold
This is a must-watch.
Peter Fonagy, known for his contributions in mentalisation-based treatment, and Bruce Wampold, the leading researching in the contextual model, debates on perennial questions in psychotherapy i.e., “Are some psychological treatments more effective than others?” “How do we become better therapists?” “What is the future of psychotherapy research?”
Key Grafs:
On Ethics:
– 4:13min: [Peter Fonagy] It is our responsibility to our patients what works and for whom the answer to that is an absolute and unequivocal yes. I would consider any attempt to hinder that process to be both unethical and unacceptable intellectually.– 8:26min: [Bruce Wampold] … How is it we keep developing new therapies and the outcomes we get with patients really have not improved over time? This is disturbing to me.
On What Makes a Difference in Outcome
– [BW cont.] …what really makes a difference is the therapists. There are some really good cognitive behavioral therapists who do a great job and when I say a great job I’m not talking abou tthey look good if you observe them. I mean, they actually achieve good outcomes with their patients.But there’s some very poor cognitive behavior therapists and with dynamic therapist, emotion-focused therapists… The key to success and you got to the epistemic trust is that some therapists have the skills to be able to help patients regardless of the treatment.
– 9:47min: [BW] The continued focus on treatment really puts the spotlight in the wrong place. regardless of the treatment. the continued focus on treatment really puts the spotlight in the wrong place. okay. It’s us—therapists who make therapy work.
On What Doesn’t Work
– 10:45mins: [BW] What doesn’t work is just sitting with the patient and beingempathic understanding okay. Treatments without structure without some way for the patient to workhard to overcome their difficulties don’t work as well as focus treatments and CBT has really taught this.– In the eating disorder area the trial that Stig Polson and colleagues did where they compared CBT to psychoanalytic therapy didn’t do as well because the patients were allowed to come in and talk about anything they wanted. It was their choice whether they talked about an eating disorder… and the difficulty is difficult so they avoided it and so did the therapist so they never worked on what the focal problem.
– 12:32mins: [PF] I think that what happens in therapy across the 1246 different kinds of psychotherapy is that there are is that if you have a decent and scientifically or empirically based a model of the client and you are actually able to say something to the client that they find helpful.– 16:30mins: [BW] I would contend that every understanding of a disorder is wrong.We will find out in 10 or 15 or 20 years every explanation you have will be supplanted by a new one..1. Not necessarily going to be a true one.What’s really important… Is that the patient accepts the explanation, ok, whether it’s evidenced-based or not.
On Clinical Supervision
– 27mins: [PF]: I’m making something it is deadly serious here, that is, unless and until we put supervision that’s based on actual clinical material rather than one’s fantasy about what occurred …unless you actually do it on what had happened it’s probably not very useful.2Well worth your time to listen to this two leading figures in our field.
- Watch: The Psychotherapy Debate with Peter Fonagy and Bruce Wampold
-
- Words Worth Contemplating:
I’ve looked at love from both sides now
From give and take and still somehow
It’s love’s illusions that I recall
I really don’t know love
Really don’t know love at all.~ Joni Mitchell, Both Sides Now, 1969.
Reflection:
Just listen. Suspend analysis. Just listen.
Joni Mitchell – Both Sides, Now [Original Studio Version, 1969]
Joni Mitchell – Both Sides, Now from the LP “Clouds”, 1969 Rows and flows of angel hair and ice cream castles in the air and feather canyons everywhere, I’ve looked at cloud that way but now they only block the sun, they rain and snow on everyone so many things
PART III
-
- Read “Against”: An Article that disagrees with the common factors conjecture.
Read this paper from authors who have a different argument on the Dodo Bird verdict.
As you read it, note down your thoughts, and why you are thinking those thoughts.
- Read “Against”: An Article that disagrees with the common factors conjecture.
-
- Read “For”: An article that argues for the common factors.
After reading the first article, read this (starting from page 9). And as you read this second article, notice how your mind shifts.
What are some of the arguments that really stand out?
- Read “For”: An article that argues for the common factors.
-
- Read “For”: An Article that argues for the relative efficacy of bona-fide PTSD treatments.
To flip things around, now read a specific meta-analysis that argues for the direct comparison of bona-fide PTSD treatment.
- Read “For”: An Article that argues for the relative efficacy of bona-fide PTSD treatments.
-
- Read “Against: An article that questions the relative efficacy of bona-fide PTSD treatments
Finally, read this rebuttal to #3.
(It’s hard, isn’t it?)
- Read “Against: An article that questions the relative efficacy of bona-fide PTSD treatments
-
- Words Worth Contemplating:
“When thinking changes your mind, that’s philosophy. When God changes your mind, that’s faith. When facts changes your mind, that’s science.”
~ John Brockman, from the Edge book, What Have You Changed Your Mind About?(My addition: When you change your own mind, that’s an opinion. When someone else changes your mind, that’s love.)Bonus:
“The best way to get a correct answer on the internet is to post an obviously wrong answer and wait for someone to correct you.”
~ Kevin Kelly.
Reflection:
As a form of self-plagiarism, this was my thoughts around specific vs. non-speciifc ingredients in psychotherapy, written at a time when I was given a chance to meditate on these things for while during my prolonged dissertation.
There were early proponents who advocated that the distinction between specific and non-specific factors in psychotherapy was an arbitrary and unnecessary distinction (Butler & Strupp, 1986). Instead of focusing on disembodied distillation of specific “active ingredients” of psychotherapy, Butler and Strupp (1986) stressed the importance of a paradigm shift and move towards a contextual model of understanding, focusing on identifying primary principles of human interactional conditions between therapist and client that ultimately promote therapeutic change.
This does not mean that therapeutic models and techniques are unnecessary and that “anything goes” (Anderson, Lunnen, & Ogles, 2010). Rather, when a believable myth (i.e., approach, rationale) is delivered in a healing context by a practitioner who not only believes in its efficacy, but is also persuasive, establishes an emotionally charged and good therapeutic alliance, the practitioner is likely to be effective, especially when he or she finds a fit with the particular client’s preferences and worldview (Frank & Frank, 1993).
Stated differently, this ritualistic process of psychotherapy engages both the practitioner and client into a shared culture of healing (Fancher, 1995).
If you would like to learn more topics that can help your professional development, subscribe to the Frontiers of Psychotherapist Development (FPD). On Frontiers Friday (FPD), we serve you directly to your Inbox highly curated recommendations each week.


Recent Comments