
Note: This is a compilation of Frontier Friday, a weekly Substack published, originally released on 16 Oct. 2021.
PART I
The topic that got me hooked into the study of development and practices of highly effective therapists, was about therapist effects.
In gist, therapist effect is the reliable differences found between therapists based on client outcomes, above and beyond modality differences.
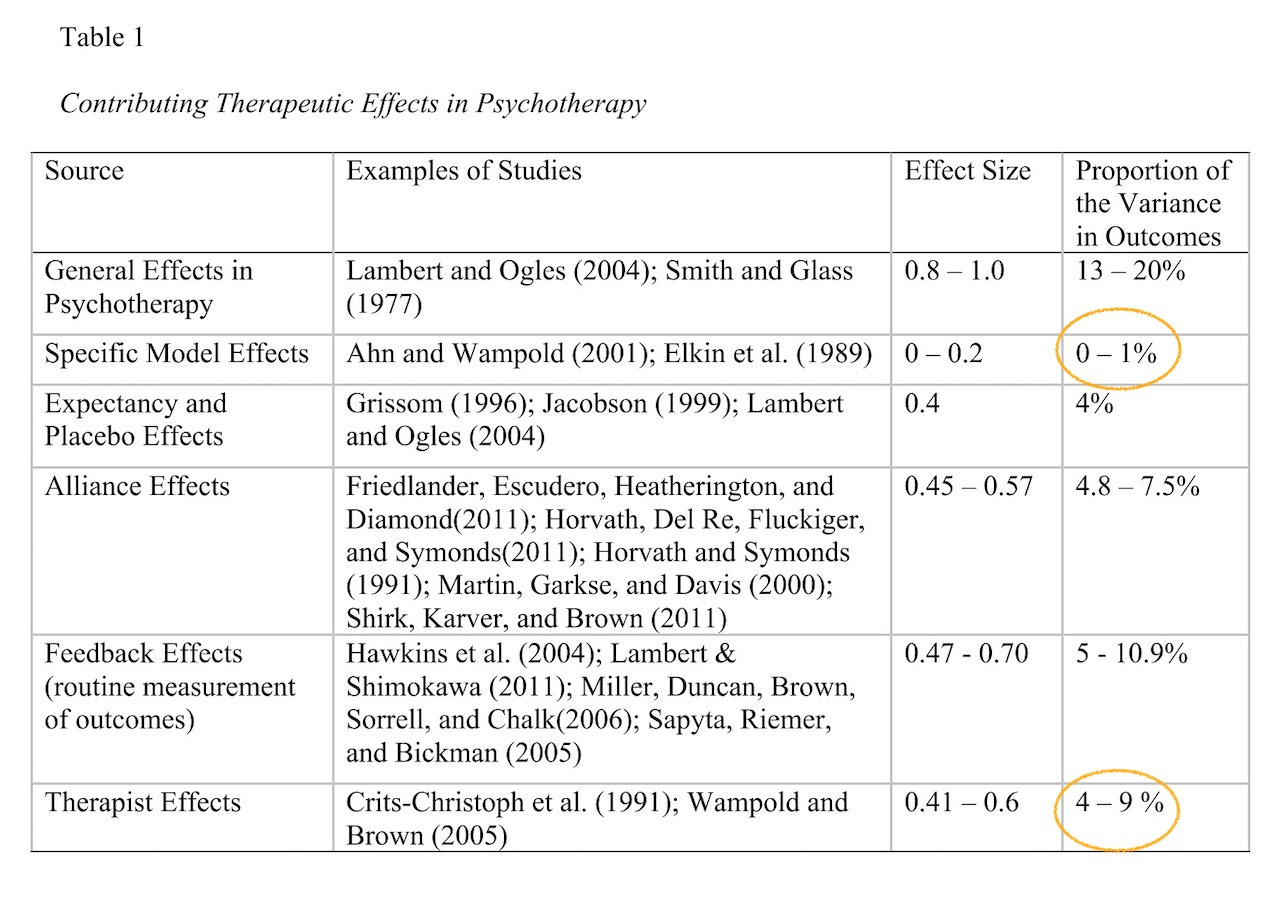
Though I did this table back in 2014, I believe this would give you an overview on the factors that contribute to outcome in psychotherapy.
Note the difference between Specific Model Effects and Therapist Effects in terms of the proportion of variance in outcomes.
Here’s the first five recommendations on this topic of therapist effects.
- 🔑 Seminal Study by David F Ricks (1974)
This seminal study was probably the first to coin the term “Supershrink.” It is also the first study to explore results obtained by therapists with different competency levels.
David Ricks compared the long-term outcomes of ‘highly disturbed’ adolescents, when the participants were later reviewed as adults, the results dramatically differed between the two therapists who provided the treatment.
For example, 27% of the first therapist’s cases received the diagnosis of schizophrenia as adults, while 84% of the second therapist’s cases received that diagnosis.
A significant amount of the adults who had seen the first therapist were more socially well-adjusted, compared to those who saw the second therapist, despite the fact that, at commencement of therapy, both therapists’ caseloads were equal in level of disturbance and other variables (gender, IQ level, socio- economic status, age, ethnicity, period seen, and frequency of psychotic disturbances found in the parents). Even though both therapists were trained in the psychoanalytic tradition, Ricks found that they differed in five major ways in which psychotherapeutic methods were employed:
i. Compared to the other therapist, the “Supershrink” allotted more of his effort to help the more disturbed adolescents, instead of those easier to treat.
ii. He also used resources external to the therapy context, and was more competent in supporting the youths’ development of autonomy, while helping parents to recognise the importance of their adolescent’s individuation.
iii. The “Supershrink” was firmer and more direct with the families and employed fewer intrapsychic interventions.
iv. He was more skilled than the “Pseudoshrink” in developing a deeper and more lasting therapeutic relationship, and
v. The “Supershrink” was keen to elicit the patient’s feedback of each session.Of course there was severe limitation by comparing with only two therapists. But this gave birth to an important research area decades later.
- ✋ Waiting for Supershrink
This 2003 study based on John Okiishi’s 200 doctoral study found that 4.1% of outcomes in a university counselling centre setting was attributable to therapist effects. Okiishi and colleagues found that “The therapists whose clients showed the fastest rate of improvement had an average rate of change 10 times greater than the mean for the sample.” Conversely, “the therapists whose clients showed the slowest rate of improvement actually showed an average increase in symptoms among their clients.”
- ⚠️ Consequence of Ignoring Therapist Effects
In this study published in Psychological Methods titled, “The Consequence of Ignoring a Nested Factor on Measures of Effect Size in Analysis of Variance” (Wampold & Serlin, 2000), the researchers stressed that ignoring therapist effects in the investigation would falsely inflate the estimates of treatment effects.
That’s because many outcome studies ignore the “nesting” nature of the statistical analysis. In other words, analyses that do not take into account the dependency of “who” the treatment provider is, is not actually representing the actual reality of treatment delivery.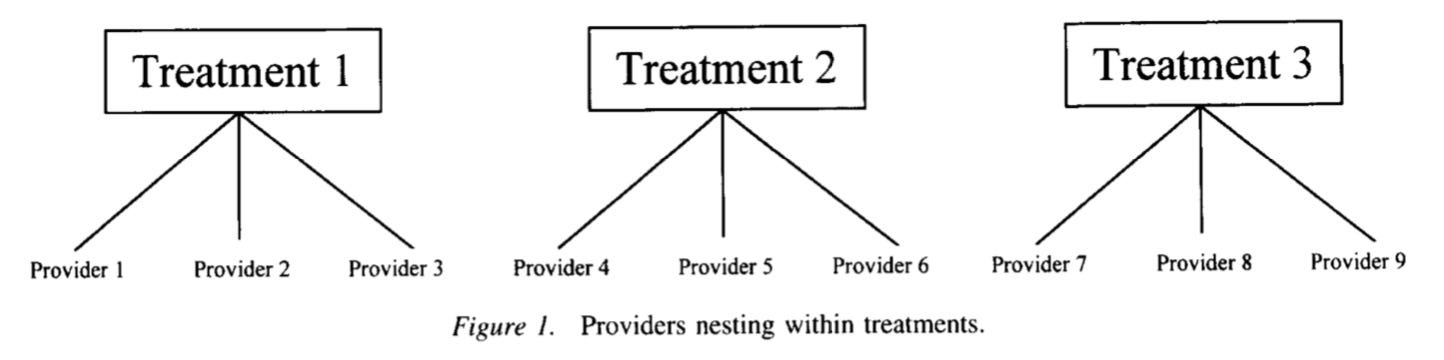
Wampold and Serlin concluded that there are “serious consequence” for ignoring who the treatment provider is.
(Sidenote: This study probably contributed to a rise in multi-leveling modeling analysis in our field). - 😱 Psychiatrist effects in the psychopharmacological treatment of depression
This study blew my mind. Taking the advice of “nesting factor” in the data, the researchers reanalysed the famous Treatment of Depression Collaborative Research Program (TDCRP) dataset by accounting for who the psychiatrist was in the prescription of antidepressants.
What did they find?
“The proportion of variance in the BDI scores due to medication was 3.4%, while the proportion of variance in BDI scores due to psychiatrists was 9.1%.” In other words, “the psychiatrist effects were greater than the treatment effects.”
What about the difference between active drug and placebo? One-third of the psychiatrists demonstrated superior outcomes with placebo than one-third of the psychiatrists demonstrated with imipramine hydrochloride.”
In other words, “effective psychiatrists augment the effects of the active ingredients of imipramine hydrochloride as well as produce benefits with a placebo.”
Isn’t that fascinating?
- ⏸ Words Worth Contemplating:
“We all want progress, but if you’re on the wrong road, progress means doing an about-turn and walking back to the right road; in that case, the man who turns back soonest is the most progressive.” ~ C. S. Lewis
Reflection:
How do we turn clinical research into me-search? Based on the above findings, what are the implications of on how we engage in professional development?
Characteristics of Highly Effective Therapists (PART II)
- 🤷🏻♂️Psychologically Minded and Expecting More
This 1996 study analysed 28 therapists in the Treatment of Depression Collaborative Research Program (TDCRP) dataset found the following:
i. The more effective therapists were more psychologically minded, as opposed to having a biological orientation (i.e., medication, electroconvul’ sive therapy),
ii. Expected more sessions than did moderately and less effective therapists.These differences were independent of the four types of treatment provided (cognitive behavior therapy, interpersonal therapy, imipramine medication plus clinical management, and pill placebo plus clinical management) or the research site. The difference in effectiveness was also not related to the therapists’ level of clinical experience.
- ✋ Who Contributes the Most to the Alliance?
We’ve all heard about the importance of working alliance. But who contributes the most to it? The client, the therapist, the fit between both parties?
In an elegant study, Baldwin, Wampold, and lmel (2007) were able to disentangle the alliance—outcome correlation, and found that the alliance formation was not due to the client, the interaction of client and therapist, nor the consequence of early improvements. Rather, the researchers found that it was largely due to the contribution of the therapist in the alliance.
In other words, therapists who, on average, are able to establish agreement on goals, tasks, and level of bond with the client (Bordin, 1979) performed better than therapists who did not form as strong a therapeutic engagement with their clients.
Rarely do we see this in social sciences, but a whooping 97% of the variance in therapists explained the formation of good alliance, as rated by clients.
Here’s a grab from Baldwin’s et al.’s paper: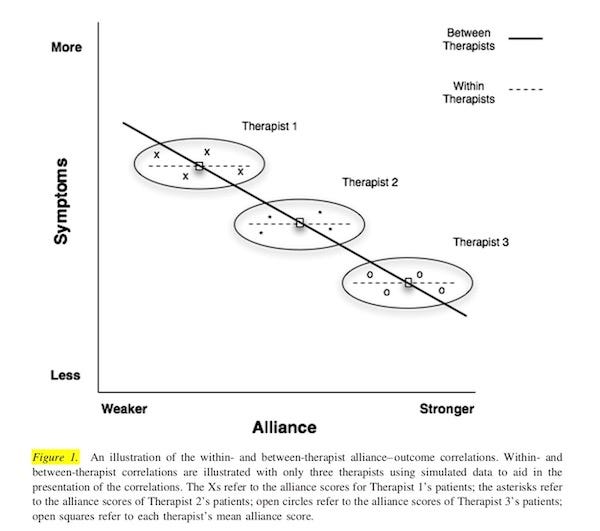
- ⚠️ Skills in Handling Difficult Interactions
A handful of studies by Tim Anderson and team have showed that the more effective therapists are reliably more able to handle difficult interpersonal situations in therapy than their peers.
They measure this with the Facilitative Interpersonal Skills (FIS) task and correlate that with therapists outcomes.
In a randomised study that my colleagues and I did in 2015 (still not yet published, I’m sorry. It’s a slow drag when I’m not in academia), we were able to improve therapist’s ability using a deliberate practice framework. Stay tuned once we can release it.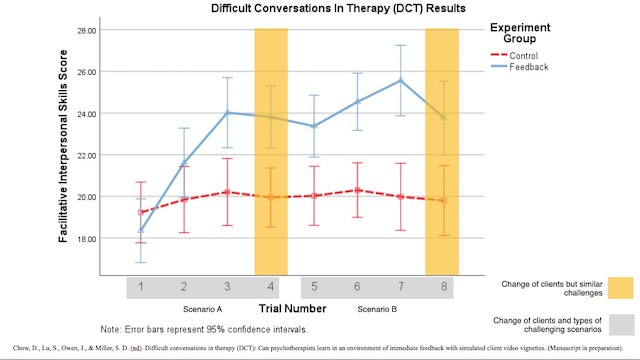
- 😱 Self-Doubt
Two studies here.
The more effective therapists seemed to. be a self-critical bunch. In the Vanderbilt psychotherapy research study, Najavits and Strupp (1994) found that effective therapists were more self-critical and reported making more mistakes than less effective therapists.
In a later study, therapist-reported professional self-doubt (PSD) was found to have a positive effect on client ratings of working alliance, with higher levels of PSD suggesting an open attitude toward admitting their own shortcomings (Nissen-Lie, Monsen, & Ronnestad, 2010).
More about Doubt.
- ⏸ Words Worth Contemplating:
“Measure what they do, not what they say.”
~ K. Anders Ericsson, personal comms.
Reflection:
We tend to default to “Working Alliance = Relationship.” Bordin (1979), however, points out that there are 3 key elements under the hood of a good relationship in therapy: 1. Agreement on goals, 2. Tasks, and 3. Emotional bond. Emotional connection is primary, but what about the therapeutic tasks and consensus of focus in therapy? How do we take care of this trifecta, since it impacts outcome dramatically?


Recent Comments